
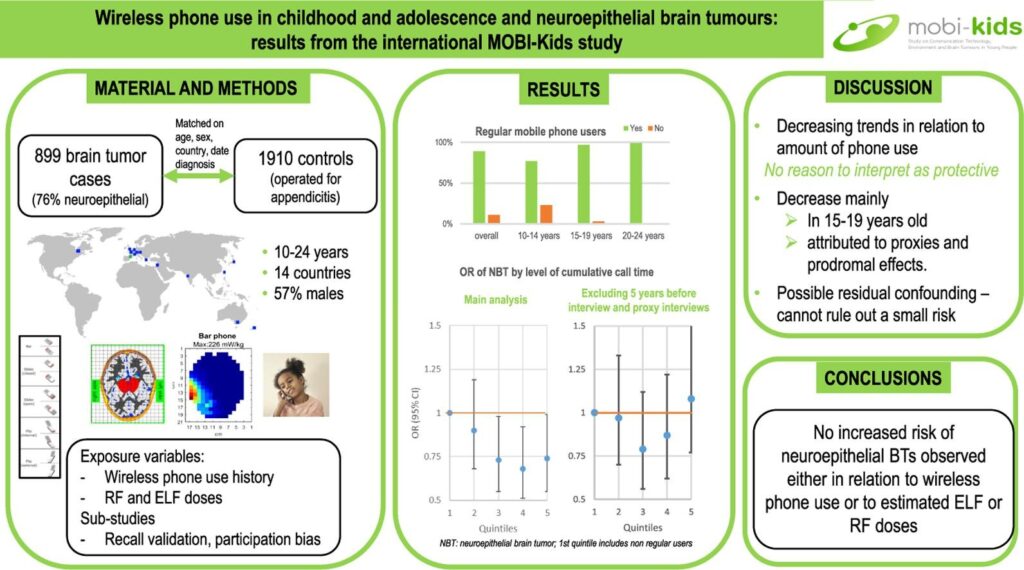
The Mobi-kids study (whose results were expected since 2016!) was finally published on December 30, 2021, in the scientific journal Environment International. Its authors conclude their work as follows:
Overall, our study provides no evidence of a causal association between wireless phone use and brain tumours in young people. However, the sources of bias summarised above prevent us from ruling out a small increased risk.
And the least we can say is that the methodology of the study as well as its results seem to us to be controversial.
[1/2] Here is a summary of our first analysis of the study, followed by the main critical points which, in our opinion, deserve to be studied further by the international scientific community.
Mobi-kids in brief
Mobi-kids is a case-control study conducted in children, adolescents and young adults to analyze the possible relationship between communication technologies, the environment and brain tumors. Mobi-kids was conducted in fourteen countries (Australia, Austria, Canada, France, Germany, Greece, India, Israel, Italy, Japan, Korea, the Netherlands, New Zealand, Spain) and was international in scope, investigating whether the use of wireless phones increases the risk of brain tumors in young people.
Mobi-kids summary results
671 tumor cases in young people recruited in fourteen countries
Between 2010 and 2015, the study recruited 899 young people aged 10 to 24 years, all with benign or malignant brain tumors of the neuroepithelial type (for 671 cases), mainly gliomas. A control group included 1,910 young people, operated on for simple appendicitis.
Even in the youngest age group, the vast majority of participants were wireless phone users, including a substantial number of long-term users (i.e., for more than ten years): 22% overall, 51% among 20-24 year olds.
One call per week for three months considered regular use
These young people with a tumor and the control group were divided into three subgroups: 10-14 year olds (287 cases, or 42.8%), 15-19 year olds (217 cases, or 32.3%) and 20-24 year olds (167 cases, or 24.9%). Most of the younger subjects had low mobile phone use, so comparing risk within each age category was feasible.
Regular phone use was defined as “having made or received calls at least once a week for a period of three months or more.” These variables were calculated separately for mobile and cordless phones.
In the 15-19 age group, non-regular users accounted for 3% of participants. In the 20+ age group, they were 1%.
Algorithms to measure level of exposure

Mobi-kids 2G 3G Wi-FI DECT ELF
The analyses of ELF (Extremely Low Frequencies) and RF ( Radio Frequencies) dose from wireless phones are based on the algorithms developed in Mobi-kds to estimate the cumulative and time-weighted average ELF-induced current density and cumulative RF specific energy absorbed at the center of gravity of the tumor of the young affected individuals.
According to the authors of the study, the algorithms took into account the entire history of wireless calls received or made by the subjects, combining reported information on the duration of calls in different time periods with the characteristics of the networks and phones indicated as having been used – since these vary in the amount and distribution of the ELF and RF dose in the brain.
The analyses are based on previous use of non-wireless phones (mobile and cordless) as reported by study participants, as well as the estimated ELF and RF dose as described above.
Other uses of mobile phones at the time of the interview were recorded: the number of text messages sent per day; the time spent (in minutes per day) sending emails, videos or files, and downloading music and movies; and the time spent using VoIP and Wi-Fi (in minutes per day).
Call duration ranging from 53 to 655 hours depending on the age of the subject
The use of wireless phones differs greatly by age (Table 2): among 10-14 year olds, 77% were regular users compared to 97% for 15-19 year olds and 99% for 20-24 year olds.
The median number of calls reported is 3,156, ranging from 1,075 in the youngest age group to 8,427 in the oldest age group (20-24 years). A similar pattern is observed for the total duration of reported calls, with a median of 177 hours, ranging from 53 hours in the youngest age group to 655 in the oldest group.
No formal analysis was conducted to account for possible differential recall bias, as the results of the operator validation study provided no evidence of differential recall between cases and controls (van Wel et al., 2021). The link to the referenced article had not yet been published at the time of the release of Mobi-kids…
Not so reassuring results
According to the study’s authors, the overall pattern of OR (odds ratios) does not suggest an increased risk of brain tumors in relation to the use of wireless devices (or mobile or wireless phones separately). Only in the youngest age group is there a possible increase in risk related to time since the start of use for temporal lobe tumors, based on a small number of cases.
However, the results do not rule out a possible accelerated growth effect of brain tumors related to wireless phone use. The authors hypothesize that many tumors found in childhood or adolescence may be generated before or shortly after birth.
Thus, tumors eligible for the Mobi-kids study would primarily peak in the third year of life and decline thereafter. Therefore, in the age range of 10 to 24 years, many tumor patients may have already harbored a growing mass of neoplastic cells leading to their brain tumor diagnosis after they started using wireless phones.
Under these circumstances, again according to the experts, the use of wireless phones could have increased the growth rate of these latent tumors and led to an earlier diagnosis.



